Question #1: Whitening vs. Bleaching
I have been trying to whiten my teeth and have bought every kind of toothpaste that says, ‘Whitening’; but none seem to work. Why is this? -J.S. New Jersey
Answer:
To understand why whitening toothpastes don’t always deliver, we have to understanding the difference between ‘whitening’ and ‘bleaching’…terms that toothpaste manufacturers would prefer that you stayed confused about!

When teeth are young, the enamel is thick and not very transparent. So as long as the surface of the teeth are free from stains and grime, the teeth will look fairly white.

If the surfaces of the teeth do have stains, then the teeth will look darker in the same way as a grimy windowpane will darken the view. In this case any toothpaste that has enough abrasives in it can polish this grime off the surface and because of that the FDA permits a ‘whitening’ claim.

But as we age, the enamel becomes thinner and more transparent, revealing the yellow color of the tooth layer under the enamel, the ‘dentin’, more clearly. To lighten this yellow color, not due to surface grime, a bleaching agent will need to be used (and all surface grime must first be cleaned away to allow it to penetrate the enamel and bleach out the dentin)
Question #2: Clicking Jaws
Why do my jaws ‘click’? -E.B. New Jersey
Answer:

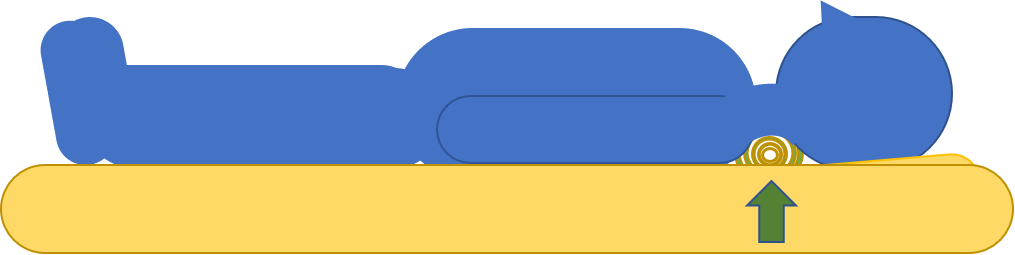
The clicking is a result of a jaw joint that has had some wear and tear. In a normal joint as pictured to the left, there is a cartilage disc that separates and cushions the ball and the socket.

Because the jaw joint not only ‘hinges’ like an elbow or a knee, but also ‘slides’ (the only joint the body that does this), the ball of the joint has to be able to slide in the socket. This happens when the disc is pulled forward by a little muscle (called the ‘internal pterygoid’). Then the ball, sitting on the disc like a child sitting on a snow sled, glides forward. In this picture you will notice that the lower teeth now touch the edges of the upper teeth as the jaw has come forward. The muscle is like the friend who pulls the rope attached to the sled.

But if the muscle pulls the disc when the jaws are otherwise at rest—a frequent problem in people who have bite problems—then when the jaw does slide forward the ball no longer sits squarely on the middle of the disc but instead starts to ride on the rear lip of the disc.

If this happens over a long period of time the rear lip of the disc gets compressed and it no longer serves to keep the ball centered on it, but rather the ball can now slip off the back of the disc when the jaw opens. This produces a ‘click’ and in early cases when the jaw closes the ball hops back onto the disc and then clicks yet again when the jaw opens again

In late stages the disc gets permanently displaced in front of the ball and then the clicking stops, but there can then be more serious TMJ problems.
Question#3: Porcelain “Fillings”
In your website you describe a replacement for cast gold restorations made with a kind of liquefied porcelain. Is this the same as ‘Cerec’? -M.M., Washington, DC
Answer:
The technology for restoring teeth with different kinds of porcelain and using different means of fabrication has grown by leaps and bounds in recent years. There are now three widely used technologies for creating tooth replacements out of porcelain: stacking, pressing, and milling.
Stacking refers to taking a porcelain powder, wetting it with distilled water to form a material with the consistency of wet sand, shaping it to the desired shape and then firing it in a kiln so that the porcelain particles fuse to each other to form a solid mass. It is an old technology that has been used to make porcelain fused to metal or porcelain fused to gold crowns for decades. It is also the technique for making highly esthetic porcelain laminates that are used for enhancing the appearance of front teeth. Because porcelain made in this way shrinks as it is fired, it cannot be made to accurately fit anything that is shaped like a hole (an ‘inlay’) as it always has to be ‘overbuilt’ in size to accommodate the expected shrinking. Any shape that sits on a surface (an ‘onlay’, a porcelain laminate, a biting surface) can successfully be built with stacked porcelain and it is the most esthetic material we have. In fact it can be combined with other techniques, although labor intensive to do so, for reasons described below.
Pressing refers to taking a porcelain ingot and melting it under high temperature and pressure and injection molding it into a three dimensional pattern of the missing tooth structure. This technique is explained in more detail elsewhere on this website. It produces restorations that have an extremely accurate fit, but the process involves many steps to accomplish and the varieties of porcelain that are available for pressing is fairly limited. Also, for highly aesthetic requirements it can be cut back to allow an overglazing with stackable porcelain.
Milling is the latest technology. It involves using a computer to create a three dimensional design of a tooth restoration on a computer screen, the data from which is fed into a milling machine that takes a block of porcelain and sculpts it down to the desired shape. When finished it is baked in an oven to harden the structure. This technology has become very popular because it involves many fewer steps then pressing and there are a wider variety of porcelains that are available that can be milled. Lately the most common porcelains to be used are either lithium disilicate or zirconium. Both of these are much harder than enamel and that translates into less breakage, but it also translates into much more wear on the teeth that come into contact with these restorations. Therefore an important step in their fabrication is the highly skilled and labor intensive polishing of the surfaces before they are glazed in the hardening step. Also, for better aesthetics, this material can be cut back to allow an overglazing with stackable porcelain.
Because so much of the work to make a milled porcelain restoration is done on a computer screen, some companies have developed machines different from the ones that they have been selling to dental laboratory technicians that dentists can purchase themselves in order to make these restorations right in their own office. One if these is the Cerec machine. In these circumstances the dentist or, more likely, a trained dental assistant handles the design work ‘while you wait’. It is marketed as a convenience to patients because the restoration is made in a single visit, as nothing has to be sent out to a dental laboratory. But without the oversight of a trained laboratory technician, there is a limit to the refinement that these office made restorations can reach. In regions of high aesthetic need, the skill and artistry of a trained laboratory technician, plus the additional equipment for cutting back and stacking porcelain, will be lacking in typical Cerec restorations. In addition, the polishing step is often avoided by painting a ‘glaze’ over the surface and baked. Studies have shown that this glaze layer wears off in about one year, exposing a microscopically rough underlying surface that can rapidly wear down the opposing teeth.
I want to thank Richard Pavlak, CDT, MDT, FNGS, the founder and director of Porcelain Plus Dental Systems of Cranford, NJ, for his expert help in answering this question.
Question#4: Mercury Toxicity
Are there peer reviewed published studies on the health effects of the mercury vapor released from amalgam fillings? -G., Wantage, NJ
Answer:
Elsewhere on this website you will find an extensive review of the whole issue of mercury toxicity. In terms of studies in the peer reviewed literature there are many. Here are just a few:
Summers, AO, Wineman, J, Vimy, MF, et al. Mercury released from dental ‘silver’ fillings provokes an increase in mercury and antibiotic-resistant bacteria in oral and intestinal flora of primates. Antimicrob Agents Chemother. 1993;37:825-834.
Siablerud, RL. The relationship between mercury from dental amalgam and mental health. Am J Psychother. 1989;43:575-587.
Lorscheider, FL, Vimy MF, Summers, AO. Mercury exposure from ‘silver’ fillings: emerging evidence questions a traditional dental paradigm. FASEB J. 1995;9:504-508.
Eggleston, et al. Correlation of dental amalgam with mercury in brain tissue. J Prost Dent. 1987; 58(6): 704-707
Vimy, et al. Maternal-fetal distribution of mercury released from dental amalgam fillings. Exper & Molec Pathology. 1990; 52:291-299.
Also, the current issue (September 2015) of the Journal of the American Dental Association includes a cover story on the effects of mercury exposure on US dentists. As all dentists wear gloves while working, the only route for routine exposure is via mercury vapor. The research found that there is a correlation between mercury exposure and hand tremor in dentists:
Anglen, J, Gruninger, E, et al. Occupational mercury exposure in association with prevalence of multiple sclerosis and tremor among US dentists. JADA. 2015: 146 (9): 659-668.
Question #5: The Dental/Medical Connection
Have you ever seen a correlation between people with autoimmune disorders and dental issues? I’ve started an immunotherapy medication for my Ankylosing Spondylitis and I have 3 cavities out of nowhere!!! Just wondering if these are related to the systemic issues in my body or more likely to the medications? Would love your insight! -S.Y., Santa Rosa, Calif.
Answer:
I often see correlations between auto immune disorders and dental issues, so you are not alone. The connections are many and they run in all directions:
An auto immune disorder can affect the body’s ability to fight infection or it may affect bone metabolism–this can lead to an increase in tooth decay or gum disease, it can also alter the flow or quality of saliva which has a direct influence on susceptibility to tooth decay particularly along the gum line.
At the same time, dental infections and diseases that are left unchecked can lead to various auto immune disorders. It is not uncommon, as an example, for a patient with severe untreated gum disease to have adult onset diabetes and when the gum disease is treated the diabetes goes away. Years ago I treated a patient who had recently been diagnosed with cardiac arrhythmia. He had not seen a dentist in almost 20 years and needed about 10 teeth extracted as well as other treatment to clean up the rest of his mouth. His arrhythmia vanished when his dental infections were eliminated. In both cases the heavy bacterial load present in the mouth led to high levels of these same bacteria circulating in the blood stream, leading to inflammation of the pancreas in the first case mentioned and in the heart in the second case mentioned.
Lastly, the medications used to treat auto immune disorders, be they non steroidal anti-inflammatory drugs, steroids, or inflammatory protein blocking drugs can each have side effects that can affect dental health. When there is a bacterial infection in the mouth, such as tooth decay or some kinds of gum disease, the body must mount a specific kind of inflammatory response to overcome that infection. If the inflammatory response is being muted by a medication, if will be easier for the bacterial infection to continue on and cause damage–such as tooth decay. The other issue, and this is common, is that oftentimes there is a side effect from medication that reduces the flow of the saliva, and this can have a dramatic effect on tooth decay.
So it is hard to answer your ‘either/or’ question without saying that most likely the answer is ‘and’–all of the above could apply. But we can often narrow down the possibilities on the basis of history. For example, if you have had a long history of being free from tooth decay and if your auto immune condition has been present for a long time then it would be more likely that the recent change in your medication had more to do with the new cavities. But if the medication is helping you then you would be best served by asking your dentist or hygienist for their advice on prevention. This often includes issues of diet, daily oral hygiene, and may require the use of a fluoride mouth rinse. In many holistic circles fluoride has a bad name, and I am not a fan of taking it systemically either in pill form or in treated tap water, but I have no problem recommending it for topical use for my patients who have auto immune disorders or limited flow of saliva.
Question#6: Receding Gums
Can receding gums be reversed? What treatments you use to restore gums? -A., NJ
Answer:
To properly address the problem of receding gums, it is first necessary to determine the cause in a particular person’s mouth. Gum recession can come about from a number of things and without figuring out why they are receding in the first place, no therapy, including surgically grafting new gum tissue onto the exposed areas, will result in a stable end result. So, Step One is finding out the cause or there may be a combination of causes in a particular area. Step Two is dealing with those causes so that the recession process comes to a halt. Only then, can there be a Step Three–if stopping the progression is not enough then what kind of remediation is possible and/or appropriate?
Gum tissue is largely dependent upon the bone that it sits on top of. If the bone goes away, often times, the gum goes away also. The places where this happens the most is on the upper front teeth, especially the upper canine teeth, but it can happen anywhere. It tends to happen here because the bone can be ‘eggshell thin’ in this region–just covering the upper front teeth with a thin shell of bone. If anything happens to this bone to break it down, the gum tissue recedes. So what can make thin bone disappear? Here are the most common things:
1. Gum disease. This is a bacterial infection of the gums and in its more invasive forms, the infection is not just of the superficial gum tissues (which results in red, puffy, and bleeding gums), but of the deeper parts of the gums that knit into the roots of the teeth and into the bone. If germs get a foothold on these tissues, the bone breaks down and it is often the case that there will be gum recession.
2. Teeth that hit too hard at bad angles to each other (a.k.a. ‘Bite trauma’, a.k.a. ‘Occlusal disease). If a lower front tooth happens to come into contact with the back of an upper front tooth before all the other teeth in the mouth come into contact (while in a jaw position where the back teeth ought to be the ones that hit first), then this upper front tooth will suffer from bite trauma. With repeated hits, this tooth will either move out of the way and look unsightly, or else it will loosen. In either case, the bone over the root on the front of this tooth will suffer from mechanical breakdown and the gum tissue over it will recede. This happens mostly on upper teeth and it can happen to upper back teeth as well. If you go to the place on this website where you can read a selection of my practice newsletters: https://www.centerforintegrativedentistry.com/for-new-patients/practice-news/ and go to the sixth newsletter, “Case 0105MS” you can read more about this cause of recession.
3. Chemical irritants. Certain items/chemicals, held between the gums and the cheek will cause gum recession given enough time. First on this list is chewing tobacco in either loose leaf form or else in the little packets. Also, though less common these days, some people put an aspirin tablet against an aching tooth (it doesn’t help, but the painful irritation of the aspirin, as it burns the gum, makes it feel as if the pain of the tooth is less).
4. Mechanical irritation. Some people brush their teeth with a hard bristled tooth brush and this can abrade and wear down the thin edges of the gums. A word to the wise: dental plaque has about the consistency of cottage cheese. A soft brush should be all you need to clean your teeth; it’s not like trying to get rust off of a car fender!
5. Systemic irritants. Any substance that reduces the blood supply to the very tiny capillaries that nourish the eggshell thin bone will cause that bone to die of asphyxiation. Cigarette smoke contains carbon monoxide, a chemical that binds up oxygen so tightly within the blood that it never makes it to the cells that it should be nourishing. In places where there is just the smallest, little blood supply–such as very thin bone–it’s only a matter of time. Marijuana smoke also has this effect as do recreational drugs that cause constrictions of the blood vessels. These include cocaine and amphetamines. Folks who use those drugs routinely have horrible gums problems.
So, first, which one or which combination of these five problems applies to any particular site of recession. Then the cause has to be eliminated, then the question is, what can be done? Sometimes, as long as the recession has stopped, we don’t have to do anything. Sometimes we cover the exposed root surface with a tooth colored filling, and sometimes there needs to be a visit to a periodontist for gum graft surgery.
Question#7:Thermograms for Dental Diagnostics
I recently had a dental thermogram which revealed an infection (which I was not aware of) on my left lower side. Do you believe in thermogram technology and can it be used to figure out the source of the infection? -B., Doylestown, Pa.
Answer:
A thermogram is a very useful diagnostic tool. It measures the heat given off by whatever part of the body is imaged. Today’s thermograms can be very precise, particularly when a structure is imaged over set intervals of time, the changes in the ‘heat signature’ of that structure reveal alot about what can be going on there.
In my view, the greatest use of thermograms is in breast imaging, particularly if there is a suspicion of cancer. Cancerous tumors cause blood vessels to grow towards them, and over time a thermogram will reveal ever ‘hotter’ zones where the blood flow has been made to increase.
How can thermograms be useful in dentistry? There are a number of reasons why a structure would image as ‘hot’ that have nothing to do with cancer. In the mouth, cancers are easier to detect visually, and a thermogram wouldn’t be as useful, but here, heat signatures most commonly reflect two different phenomena that also heat tissues up: infection and hyperactive muscles. So, if using a thermogram in dentistry it is most important to use other diagnostic criteria to differentiate between these two as both infection and hyperactive muscles can feel like the same kind of thing.
Recently a patient of mine brought me in a thermogram of her lower jaw, and she was told by the doctor who did the imaging that it showed an infection in the bone. She asked me to evaluate it. I looked as the history of the teeth and gums in this region of her mouth to see if I had, in the past, noticed any problems that could lead to a future infection. Finding none I then went to look at the thermograms that had been taken at different angles of her jaw (head on, side view, and looking upward from under the chin). If the hot spot seen in the side view was from within her jaw bone, it would stay in the same location in each view, but if the hot spot were from a hyperactive muscle, and this patient was a ‘clencher’, then the hot spot would move around more. To visualize what I mean, think of it this way: if I warmed up a little plastic disk and glued it to your cheek and then took the three thermogram views that I mentioned, the front view would show the hot spot far to the outside of the jawbone; the side view would show the hot spot directly over the jaw bone, and the view from below would show the hot spot at a distance away from the jaw bone.
In this way it is possible to differentiate between heat in a tight muscle, or heat in the jaw bone itself. That’s the biggest thing that is often missed, but without knowing a history of the teeth, gums and the jawbone in the imaged area it would still be impossible to be completely accurate with just a thermal image alone. There are tumors that can grow in the jaws, many of which are benign, but they can still register as hot. There can be unusual blood vessel formations, known as ‘A-V malformations’ that can image as hot without there ever being a tumor or an infection.
Still, I am fond of thermograms as a diagnostic tool. It can be the deciding factor in pinpointing which tooth is causing pain when a patient can only point to an ‘area’.
Question #8: The Dental/Medical Connection, Part II
About 3 years ago my dentist replaced all of my composite fillings with amalgam. About 2 or 3 months after that, I developed burning pains in my head, unexplained hair loss, food intolerances, etc. I asked my dentist about this and he said I could have triggered shingles. I still have all of these issues and he is not a very easy person to talk to about my concerns as believes anyone that is against amalgam is clueless, as it has no harmful effects.
I am worse off now than before I had this work done. I now clench my jaw while sleeping, my teeth have shifted, and I have cracked a lot of my enamel by doing such things.
Is it even possible to have these amalgams replaced? I am only 26 and my funds are limited. -L., Cliffwood, NJ
Answer:
Elsewhere on my website there is information about dental amalgam. While it is possible that the symptoms you describe could all be attributable to the mercury that you were exposed to as a result of the placement of your mercury amalgams, it is only a speculation based on the timing of the treatment and the timing of your symptoms. There are typically two ways to approach this: one way is get tested for mercury toxicity and my office can refer you to a number of healthcare practices where you can get that done. Yet, I have many patients who, knowing their own body, are quite certain that their exposure to mercury created specific health problems. I perform autonomic response testing to gauge the level of stress that mercury fillings are placing on the body (this is an adjunct test in my overall diagnosis and is not the same as the deeper kinds of tests that can be done).
That being said, mercury exposure can cause the symptoms that you describe in susceptible individuals and I have not heard of the shingles virus causing any of them. Regarding your clenching and shifting of teeth, this could be a result of the new fillings, regardless of what they are made of, having changed your bite in a way that is uncomfortable for your jaw muscles. That is something that a careful bite evaluation would reveal. The cracking of your teeth is likely from a combination of the extra bite stress of clenching coupled with the fact that as dental amalgam ages, it tends to expand, thus stressing the tooth structure. But, let me assure you that in almost every case it is possible to preserve teeth, even if there is very little natural tooth structure remaining.
Many of my patients are on limited budgets and I tell all of them that the first and most important step is to get a comprehensive exam and a priority based treatment plan that is designed to address the most serious problems first. That way, even if the treatment needs to be spread out over a number of years, we are always ‘putting out the biggest fires’. Feel free to call our office if you have further questions about your specific needs.
Question#9: On Root Canal Therapy
|
I have several old root canal with crowns, some have been treated more than once. I have been recommended to have the teeth removed and replaced with implants. What are your thoughts about this? –C.O., Denville, NJ |
Answer:
Elsewhere on my website you will find my approach to root canal therapy. It is and can be a valuable way to save teeth and, when done expertly and with non-toxic materials it can be successful, according to studies, about 93% of the time. This is in line with the success rate of dental implants, so either work well, most of the time. On some occasions, circumstances favor root canal treatment, in others, the balance goes to implants. There are too many factors to make general statements in this kind of forum. In your particular case, the question is: are the current root canal teeth with crowns working well for you? Or, are you having pain, swelling, or unusual health symptoms that can be traced by various means (acupuncture meridians, muscle testing) to these teeth? Just because teeth have been treated with root canal therapy, even ‘some more than once’ is not a reason in itself to go through extractions, bone grafts, implant placement and new reconstructions. But, if there are either ‘signs’–for example, evidence on dental x rays of growing areas of bone loss at the tips of the roots of the treated teeth; or ‘symptoms’–pain, swelling, discomfort chewing, recurrent sinus infections with no apparent sinus problem–then it should be investigated and the treatment you mention could very well be a step towards improved quality of life.
Question #10: The Fluoride Question
Fluoride is a patch on public health where there is an over consumption of sugar and simple carbs (white bread, crackers, pretzels, cookies, cake, etc). I am not against topically applied fluoride or, if needed, fluoride in toothpaste—but I don’t put it in the toothpaste that I have developed. The problem in my view of water fluoridation is threefold: 1. The dose varies depending on how much water a person drinks and can’t account for other sources of consumed fluoride (fruits and veggies grown in fluoride rich soil), 2. It can’t account for the different rates of absorption—which can be particularly high in ectomorphs (tall, skinny with hyper flexible joints—known in homeopathy as the ‘Calc Fluor type’). 3. Once consumed it gets into the bones of the skeleton and never leaves, ie if you get too much, it’s in there for good, and it does make bones more brittle—something that can be a problem for the elderly with things like hip fracture.
The best is not to fluoridate the water and eat healthy and practice good hygiene. But I admit that in the face of poverty and ignorance— in regions with historically high levels of decay from poor diets including drinking a lot of soda (in Appalachia they like Mountain Dew, which has a very low pH, making it a more potent destroyer of teeth), then water fluoridation is better than kids losing their teeth by the time they are 20! In ‘war zones’—different measures apply.
Question #11: Dental Detective Work
I had two mercury fillings replaced by a holistic dentist. They were replaced with some kind of amalgam I believe. They are my two upper back molars. I also had a lower molar root canal extracted (same side). This was about 2 years ago. Recently I started tasting metallic taste in my mouth. It seems like it’s coming from one or both of the replaced fillings. It’s very extreme when I’m around sheetrock or plaster dust (we are renovating a home) and it almost feels as if there is some kind of metallic chemical reaction happening. Have you heard of this or know how i can address this? Thank you! –C.L., Glen Ridge NJ.
Answer:
It will probably take some detective work to answer this question, so this will not be the final word. Yet, this question raises some interesting issues that are worth sharing in this kind of forum. First of all, if you had a holistic dentist replace mercury fillings, he or she would not have used an ‘amalgam’, as that is just another word for mercury fillings. More likely would be replacement with ‘composite’–which is a kind of high strength plastic material. If, in fact, all of the mercury fillings were removed, not leaving in any of them this material in the deeper parts of the tooth (with, for example, just a replacement of a ‘veneer’ of composite on the surface), then neither of these fillings could be the cause of the metallic taste. Also, if you had a tooth treated with root canal therapy and that tooth was extracted, it could not be the cause of this taste either. This leaves many, many open questions… Do you have any other mercury fillings in your mouth? Do you have any other metals in your mouth as a result of crowns, bridges, removable appliances, orthodontic wires, etc? The first place to look would be any metal in your mouth. If you don’t have any metal in your mouth, then there are some dental conditions and some medical conditions that can lead to a metallic taste. Poor oral hygiene is a common cause–so, are you good about brushing and flossing daily? Any sinus infection can cause a metallic taste. Certain prescription medicines and certain nutritional supplements can cause a metallic taste. Certain medical problems can also cause a metallic taste. But the clue that you give about this being triggered by work with drywall or plaster adds an interesting twist. Drywall and plaster contain calcium sulfate and the sulfur component can vary in concentration, sometimes in drywall being quite high. It was discovered some years ago that as the sulfur outgassed, it caused copper pipes near to it to corrode. Sulfur is a highly reactive element that causes the breakdown of other metals, so if there are metal ‘things’ in your mouth and you are inhaling a sulfur containing dust, you could be getting a chemical reaction that would give you this taste. That’s about as far as I can go with just this information–good luck!
Question #12: Recent Cold Sensitivity
I recently developed some severe sensitivity to cold on my teeth. Cold air and cold drinks really set them off. I brush my teeth daily and try to take really good care of them and I have not had a cavity in years. What could be causing this? –A.S. Union, NJ
Answer:
Although sudden cold sensitivity can indicate tooth decay near a nerve and even be an early warning sign that root canal therapy is needed. Far more often the cause of this problem is a combination of two separate processes. Either may be the culprit alone or there may be both at work. The processes are: Abrasion and Erosion.
Abrasion happens because there is a mineral called ‘silica’ that is a component of every toothpaste on the market (except my new toothpaste, “Dr Shuch’s Remarkable Edible Toothpaste“) and it is harder than tooth enamel and tooth dentin, the two minerals that make up every tooth. Because it is harder, every time you brush your teeth with a silica containing toothpaste, you are doing the equivalent of ‘sanding’ your teeth with very fine sand paper. It is used to abrade off stains, but particularly if you have gum recession and have exposed roots, they abrade at a much faster rate than does enamel because they are softer than enamel. It is not an unusual story for me to hear that a patient comes in and tells me, “My teeth were becoming sensitive, so I worried that I was getting a cavity and began brushing my teeth five times a day, but the problem is only getting worse!” Well, the answer to this kind of sensitivity is to stop brushing with a silica based toothpaste. Even if you don’t have my product, just brushing for a few days with just warm water will keep the teeth reasonably clean and allow the naturally calcium rich ions in saliva to harden up these root surfaces and the sensitivity should go away. Likewise, there is silica in chewing gum, that gives it a stiff, rubbery consistency. It can wear the biting surfaces of teeth down to the point that any biting pressure will give a sudden, sharp pain and these teeth will also become sensitive to cold and air. Here, the answer is to stop chewing gum!
Erosion happens from eating or drinking foods that are acid (sour). The common ones are vinegar, like what is in salad dressing or in pickles; citrus, such as lemons, grapefruits and oranges; or with some stomach conditions where there is gastric reflux or vomiting. Also, some soft drinks have a low pH that makes them taste ‘tart’ and these will cause alot of enamel erosion! Here, the thing to do is to identify the cause and reduce your consumption of it or your habit. An interesting combination of these two processes comes about when people chew citrus flavor chewing gum. It contains citric acid to make it a bit tart and it contains silica that wears down enamel. For those who chew this kind of gum for hours every day, they can can a very particular kind of wear on the teeth that can be extremely sensitive. It will look like the cusp tips of the lower teeth all have little indentations at the tips. Here, the enamel has been abraded down so that the cusp tips just contain exposed dentin, and this dentin then wears down faster than the surrounding tooth structure. So the cusp tips each will have a little cupped out area that can hurt like a knife when biting on sweet or sour foods. Sometimes we have to fill these ‘potholes’ in to make the sensitivity go away, other times, stopping the erosion will allow the teeth to absorb calcium in these areas and they will become free of symptoms all by themselves.
Question #13: Dr. Shuch’s Remarkable Edible Toothpaste
I would like to order Dr Shuch’s Remarkable Toothpaste, how can I get it? -N.A. Aurora, Co
Answer:
If you’d like to order a single tube, please use this link that will take you right to the page on Amazon. As most people have “Prime,” its less costly if you are buying a single tube to get it there and for that reason my office does not ship single tubes. But for bulk orders in multiples of 9, our office sells and ships them directly at a substantial discount from what is offered on Amazon. If you wish to order in bulk, feel free to call our office at 973-579-7400 on Mondays, Tuesdays, or Thursday’s. Pam or Suzanne will let you know what the current bulk discounts are and can help you with your purchase.
Question #14: A Bite Problem with Pain
|
I have had excruciating pain in my right ear for four months. I believe it’s because my bite is not correct. It almost feels like I have a cavity that was never smoothed down and I only bite down on my right side. I have gone to the dentist and got an appliance and it just made it worse. I am desperate to find a solution. Can you give me some advice? Who I should go to for help at this point? Thank you so much, -D., Murrieta, Ca Answer: This could be a few different things so it will need to be looked at by a dentist who has some understanding about this; more about that in a minute. Here are the most likely possibilities: If the tooth was recently filled then the most obvious thing might be that the bite on the filling is high. This is most common when the tooth is the upper last molar, as it is the tooth that is closest to the jaw joint and pain in this tooth can feel like pain in the joint. But there are other reasons besides being close to the joint why this tooth can feel like or lead to what we call ‘TMD’ or ‘tempro-mandibular dysfunction. When the bite is high on a tooth this close to the jaw hinge, then even a tiny bit of excess height can be a huge pain generator. The mechanics of this are kind of like a nut cracker. If you want to exert the maximum pressure on a walnut shell, you want to get the nut as far into the jaws of the nut cracker as you can, because that is where you’ve got the most leverage. Just like that example, you can exert the highest amount of biting pressure on the teeth furthest towards the back of the mouth. So if you have a high bite back there, you’ve got the strength of all of your most powerful muscles clamping down on that high spot. Here is how that problem can get worse in a hurry. Every tooth sits in a bony socket and is connected to the bone by millions of very short fibers, not unlike how a peach pit in a ‘cling’ peach is attached to the flesh of the peach. These fibers are actually ligaments that hold and suspend the tooth and cushion it during chewing, but if they get over-compressed they swell. This has the effect of raising the tooth up in the socket, which makes the bite problem even worse!!! The bite does not necessarily have to be high in a straight up and down bite; it can be high when you go through a chewing motion. In that case the lower tooth that engages with it will contact not the deep valley in the center of the tooth, but the slopes of the valley walls. Many dentists only check the bite in an up and down motion and don’t check to see if side-to-side movements are ‘premature’ or ‘free.’ There are other possibilities also. The problem tooth may have an infection and may need root canal therapy or the jaw hinge could have been strained from holding your mouth open for an extended period of time. These other issues would need to be ruled out, but my bet would be on first looking into the bite issue. My recommendation would be for you to go to a website run by the L. D. Pankey Foundation (www.pankeydentist.org). This is a post-graduate educational organization that teaches dentists the the art and science of getting patient’s bites correct. Unfortunately, this is not an area of education that is given much emphasis in dental school, so it is up to dentists, after they graduate and if they have this interest, in getting post graduate training in this area. They also teach dentists how to properly make bite appliances as there are many different kinds and the wrong kind can make a problem worse. There are a few “schools of occlusion” that teach these skills, but Pankey is the best! I went on their site and plugged in your city and there are four dentists all within about one hour of you. Good Luck!!! Question #15: Thermography Part II Do you use thermography in your practice? I have not been able to find a single dentist in Central Europe who is even familiar with it. I tend not to trust normal x-rays. -M.L. Germany Answer Thermography is a valuable diagnostic tool especially when it comes to evaluating areas of inflammation or infection. It captures the ‘heat signature’ of muscles and bones and in this way I can often use it to differentiate between pain coming from a jaw infection or pain coming from an overlying inflamed muscle. It gives different information than an x-ray; one does not replace the other. Most dentists are not familiar with them and don’t know how to read them. But I have encountered MD’s that also do not understand how to interpret head and neck thermograms properly. I don’t have a thermography camera, but I send patients to local medical offices that typically use them for breast imaging in lieu of annual mammograms. You could likely find an office that can image your head and neck that way, but finding a practitioner who can interpret it may be a challenge and again, the imaging does not replace x-rays. Question #16: Careful Mercury Removal Protocol Do you follow a protective protocol for amalgam removal? -J. Montclair, NJ Answer I’ve developed and refined a amalgam removal protocol that has patients coming to me from all over the country. On this same website, go to this page to view my approach: and go to this page to view my recommendations for patients prior to having their amalgams out. Question #17: On Laser Assisted Gum Surgery
|